Undiagnosed vEDS revealed as cause of man’s perforated colon
Case study documents road to 25-year-old's diagnosis



A 25-year-old man’s perforated colon was the result of an undiagnosed case of vascular Ehlers-Danlos syndrome (vEDS), according to a case study from Portugal.
“In the absence of colonic disease and with clinical manifestations of connective tissue disorders, a genetic investigation for vEDS should be conducted, even in individuals without a family history,” the researchers wrote. Centralized care, with experts and multiple specialists, can help in “complex cases,” they wrote.
The study, “Ehlers-Danlos syndrome and the risk of spontaneous colonic perforation: clinical insights and surgical implications,” was published in the Journal of Surgical Case Reports.
Ehlers-Danlos Syndrome (EDS) is a group of genetic conditions that affect connective tissue, which supports and gives structure to skin, joints, blood vessels, and other organs. Hallmark features include unusually mobile joints that easily dislocate and soft, stretchy skin. Of the 13 recognized types of EDS, vEDS is considered the most severe due to weakness in blood vessels and carries a high risk of severe bleeding, which can be life-threatening.
Spontaneous gastrointestinal perforation — a hole in the digestive tract — is the most frequently observed digestive complication in vEDS, with the colon most commonly affected.
A complicated case
The man described in the report arrived at the emergency department with sudden, widespread, intense abdominal pain. He had a history of attention deficit hyperactivity disorder, which was managed with medication; repetitive shoulder dislocations; and smoking. His mother had died at a young age from an “unclear acute gastrointestinal event,” the researchers wrote.
Physical examination showed a rigid abdomen with widespread tenderness, and blood tests revealed elevated biomarkers of inflammation. CT scans found air pockets in the abdomen and free fluid around the pelvis.
An exploratory laparotomy, a surgical procedure in which an incision is made through the abdominal wall, discovered a perforated colon with fecal matter in the abdominal cavity. Doctors performed a colo-colic anastomosis, a surgical procedure in which two segments of the colon are joined together after the affected portion is removed.
The man was transferred to the intensive care unit, where he developed severe lower back pain and high blood pressure that didn’t respond to medication. A CT scan revealed blood vessel blockages in his left kidney due to blood clots. He was treated with antibiotics and blood thinners. Despite these measures, he continued to experience further blood clotting events in the left arm and right lung. A battery of tests ruled out several conditions related to blood clotting.
Angiography — an imaging technique used to visualize blood vessels — revealed microaneurysms, small, balloon-like bulges in the blood vessels of the liver, stomach, and tissue around the intestines. Doctors suspected polyarteritis nodosa, an inflammatory blood vessel disease, and the man was discharged from the hospital three weeks after surgery, with blood thinners and steroids.
Less than a week later, he returned to the emergency department with lower abdominal pain and nausea. Blood tests revealed high levels of white blood cells, a sign of body-wide inflammation. A CT scan found free fluid and free gas bubbles next to the previous surgical site.
Another exploratory laparotomy found a large pool of blood on the wall of the left colon, but no signs of perforation. After draining the excess fluid, doctors performed an ileostomy. This surgical procedure creates an opening in the abdomen, bringing the end of the small intestine to the surface of the skin.
Further CT scans confirmed decreased blood pooling on the colon wall, but showed signs of a fistula, a connection between two body parts that don’t normally connect. After he was stabilized, the man was discharged from the hospital with home care, including an abdominal drain, parenteral nutrition (feeding directly into the bloodstream), antibiotics, and a gradual reduction in the steroid dosage.
The man returned to the emergency department, where he was diagnosed with an enterocutaneous fistula — an abnormal connection between the gastrointestinal tract and the skin —and readmitted. He received parenteral nutrition for almost two weeks, which reduced the fistula output and improved his clinical status. He was again discharged, tolerating an oral diet and with a functioning ileostomy.
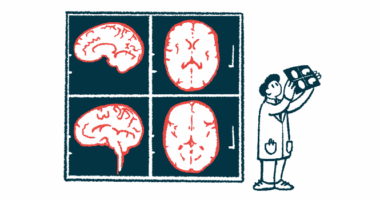
A follow-up neurological examination via MRI revealed leukoencephalopathy, a disorder that affects white matter in the brain. Subsequent genetic testing detected a mutation in the COL3A1 gene, the cause of vEDS. An MRI of the left shoulder showed signs of a bone defect related to the shoulder dislocations.
“In this case, multidisciplinary management involving surgeons, physicians, and genetic counseling was required,” the researchers wrote. “Centralizing care at specialized centers is beneficial in order to provide the expert monitoring that such complex cases require.”